According to the Department of Health, long-term conditions are ‘those conditions that cannot, at present be cured but which can be controlled by medication and other therapies’.
A long-term conditions health needs assessment was undertaken in 2014-15 which looked in detail at the eight long-term conditions. A brief overview of these conditions and how many people are affected in Devon is supplied below.
Coronary Heart Disease (CHD)
Coronary Heart Disease (CHD) is when coronary arteries (the arteries that supply the heart muscle with oxygen-rich blood) become narrowed by a gradual build-up of fatty material within their walls. 29,932 people were on a GP disease register for the condition in Devon in 2015. The expected number of people with the condition is 43,759, suggesting that around 68% of the people who are likely to have the condition are on the GP disease register.
Heart Failure
Heart failure is a condition caused by the heart failing to pump enough blood around the body at the right pressure. It usually occurs because the heart muscle has become too weak or stiff to work properly. 6,364 people were on a GP disease register for the condition in Devon in 2015. The expected number of people with the condition is 13,286, suggesting around 48% of the people who are likely to have the condition are on the GP disease register.
Stroke
This definition includes stroke, a serious medical condition where one part of the brain is damaged by a lack of blood supply or bleeding into the brain from a burst blood vessel, and transient ischaemic attack (TIA), a temporary fall in the blood supply to one part of the brain, resulting in brief symptoms similar to stroke. 17,756 people were on a GP disease register for the condition in Devon in 2015. The expected number of people with the condition is 19,154, suggesting around 93% of the people who are likely to have the condition are on the GP disease register.
Chronic Kidney Disease (CKD)
Chronic Kidney Disease (CKD) is a long-term condition where the kidneys do not work effectively. 31,055 people aged 18 and over were on a GP disease register for the condition in Devon in 2015. The expected number of people with the condition is 73,114, suggesting around 42% of the people who are likely to have the condition are on the GP disease register.
Diabetes
Diabetes is a condition where the amount of glucose in blood is too high because the body cannot use it properly because the pancreas doesn’t produce any insulin, or not enough insulin, to help glucose enter your body’s cells, or the insulin that is produced does not work properly (known as insulin resistance). 41,114 people aged 17 and over were on a GP disease register for the condition in Devon in 2015. The expected number of people with the condition is 53,733, suggesting around 77% of the people who are likely to have the condition are on the GP disease register.
Asthma
Asthma is a common long-term condition that can cause coughing, wheezing, chest tightness and breathlessness. The condition is marked by attacks of spasm in the bronchi of the lungs, causing difficulty in breathing. It is usually connected to allergic reaction or other forms of hypersensitivity. 50,592 people are on a GP disease register for the condition in Devon. The expected number of people with the condition is 71,853, suggesting around 70% of the people who are likely to have the condition are on the GP disease register.
Chronic Obstructive Pulmonary Disease (COPD)
Chronic Obstructive Pulmonary Disease (COPD) is the name for a collection of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways disease. People with COPD have difficulties breathing, primarily due to the narrowing of their airways, this is called airflow obstruction. 14,542 people are on a GP disease register for the condition in Devon. The expected number of people with the condition is 21,405, suggesting around 68% of the people who are likely to have the condition are on the GP disease register.
Epilepsy
Epilepsy is a neurological disorder marked by sudden recurrent episodes of sensory disturbance, loss of consciousness, or convulsions, associated with abnormal electrical activity in the brain. 5,397 people aged 18 and over were on a GP disease register for the condition in Devon in 2015. The expected number of people with the condition is 7,394, suggesting around 73% of the people who are likely to have the condition are on the GP disease register.
Age, Sex and Inequality Summaries
The above summary uses information from the GP registers and estimates of prevalence from national studies to provide a profile of long-term conditions in Devon. The following analysis uses data from a project in Somerset, to provide further information about the pattern and costs of long-term conditions across the health and social care system. The South West Academic Health Service Network launched the Symphony project in Somerset, which joins up health and social care data so usage and cost of services across the whole system can be analysed. The project is expected to be extended to cover Devon in due course, but the existing Somerset data can still deliver some useful insights for our local population. This can be done by applying the patterns seen by age, sex and social characteristics in Somerset to our local populations to estimate what we might expect to see in Devon.
Figure 9.24 provides an overview of each of our selected conditions from the Somerset Symphony project, applied by age, sex and deprivation to the Devon population. The column ‘estimated treated prevalence’ as the Symphony project captured the numbers recorded with disease either in primary care, secondary care or elsewhere in the health and social care system. The subsequent charts for each condition show the profile by sex, age and deprivation. Most conditions are more likely in males than females, in older age groups, and in more deprived areas. The following patterns are seen:
- For the pattern by sex, only Asthma has higher prevalence in females. The conditions where male rates are particularly higher are CHD (86% higher), CKD (52% higher) and Heart Failure (51% higher).
- The pattern by age, highlights an increasing pattern with age, with much lower likelihood of having the condition in younger age groups for cardiovascular diseases (CHD, Stroke and Heart Failure), along with CKD. A similar pattern is seen for COPD and diabetes but the peak in earlier in old age (80 to 84) and prevalence rates drop of more quickly for older age groups. Asthma peaks at an earlier age (20 to 24), whilst Epilepsy prevalence is much more even across adult age groups.
- For all conditions prevalence rates are higher in more deprived areas. The greatest differences are seen for COPD (134% higher), Epilepsy (81% higher) and Diabetes (78% higher).
Figure 9.24, Estimated number treated for selected long-term conditions in Devon, with summary breakdowns by age, sex and deprivation, 2013-14 (Somerset Symphony data applied to wider Devon, Plymouth and Torbay population profile)
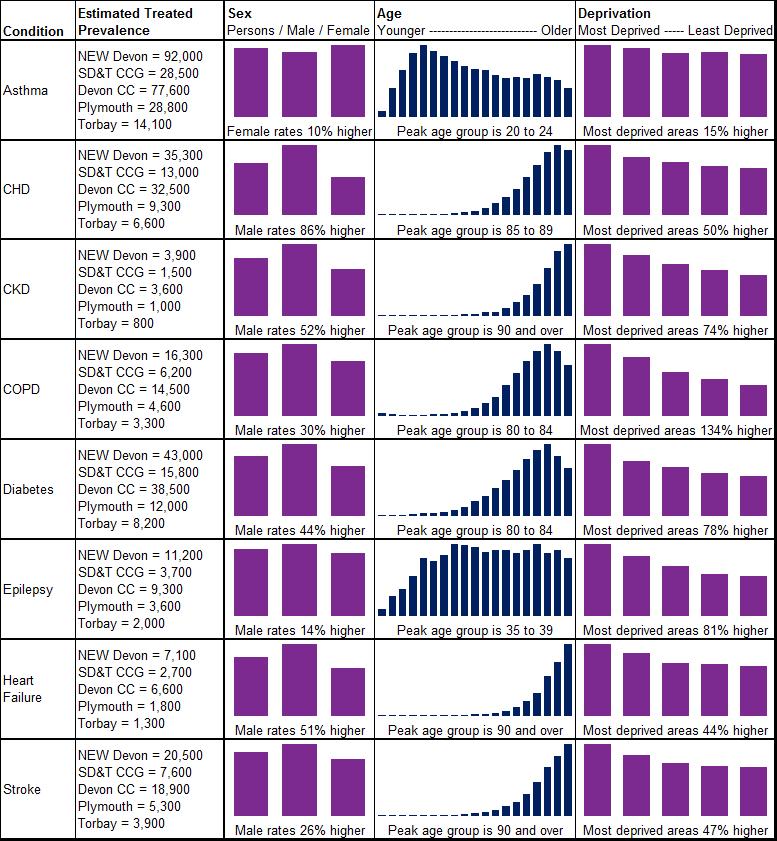
Source: South West Academic Health Science Network, Symphony Project Data for Somerset modelled by age, sex and deprivation for the Devon population, 2014
Figure 9.25 looks at the estimated overall health and social care costs of selected long-term conditions (green circles) in the Devon County Council area, and how much of this cost can be attributed to the higher prevalence of these conditions in more deprived areas (red circles). This helps us quantify the cost of health inequalities, and also highlight the conditions with the greatest variation and potential for reduction through a focus on prevention (blue circles). This analysis used unit costs for the conditions by service and age were taken from the Symphony Project and then applied to the estimated treated prevalence by age figures. The conditions with the highest overall costs are CHD (£64.7m), Stroke (£52.4m), Diabetes (£45.9m), and Asthma (£43.6m). The highest levels of excess cost due to higher prevalence in more deprived areas were COPD (£7.1m), In terms of percentage share, the greatest potential savings through prevention and reducing prevalence in more deprived areas is seen for COPD, Diabetes and CHD. This is illustrated by COPD costs, which are estimated to total around £23.3 million in Devon, but if all areas had the same prevalence as the least deprived areas, then the cost would be around £7.1 million lower at around £16.2 million. These figures may also be an underestimate as average cost for all persons by service and age is used, and the service costs for those living in more deprived areas is likely to be greater.
Figure 9.25, Estimated Health and Social Care System-Wide Cost including overall, health inequality related and opportunity costs for selected long-term conditions, Devon County Council, 2014
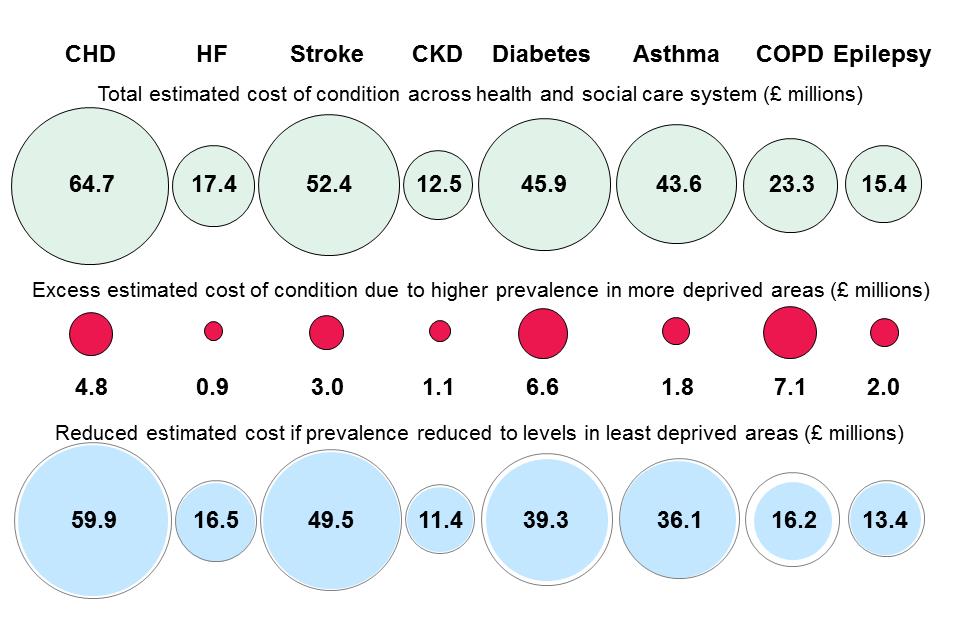
Source: South West Academic Health Science Network, Symphony Project Data for Somerset modelled by age, sex and deprivation for the Devon population, 2014
Table 9.10 reveals the number of hospital admissions where the primary diagnosis was for one of the selected long-term conditions locally. The greatest volumes of hospital admissions were seen for COPD (around 4,000 admissions), Stroke (around 2,100 admissions) and COPD (around 1,650 admissions).
Table 9.10, Number of hospital admission for selected long-term conditions (primary diagnosis only), for CCGs, NEW Devon localities and upper tier / unitary local authorities in Devon, Plymouth and Torbay, 2013-14
| Condition | Admission Type | South Devon & Torbay CCG | NEW Devon CCG | Eastern Locality | Northern Locality | Western Locality | Devon County Council | Plymouth City Council | Torbay Council |
| Asthma | Elective | 14 | 183 | 6 | 167 | 10 | 184 | 7 | * |
| Emergency | 302 | 783 | 347 | 181 | 255 | 702 | 208 | 172 | |
| Other | * | * | * | * | * | 6 | * | * | |
| CHD | Elective | 451 | 1994 | 797 | 544 | 653 | 1770 | 465 | 201 |
| Emergency | 773 | 2309 | 902 | 505 | 902 | 1983 | 666 | 426 | |
| Other | 41 | 245 | 56 | 165 | 24 | 248 | 15 | 24 | |
| CKD | Elective | 118 | 323 | 172 | 55 | 96 | 301 | 71 | 62 |
| Emergency | 28 | 96 | 32 | 17 | 47 | 76 | 28 | 17 | |
| Other | * | 7 | * | * | * | 11 | * | * | |
| COPD | Elective | 36 | 214 | 72 | 23 | 119 | 129 | 104 | 16 |
| Emergency | 627 | 1693 | 679 | 325 | 689 | 1413 | 572 | 340 | |
| Other | 78 | 68 | 23 | 25 | 20 | 112 | 6 | 28 | |
| Diabetes | Elective | 15 | 65 | 27 | 13 | 25 | 56 | 18 | 6 |
| Emergency | 217 | 615 | 229 | 74 | 312 | 446 | 279 | 112 | |
| Other | 13 | 25 | * | 15 | * | 30 | * | * | |
| Epilepsy | Elective | 31 | 144 | 33 | 27 | 84 | 106 | 58 | 9 |
| Emergency | 202 | 605 | 183 | 135 | 287 | 468 | 217 | 115 | |
| Other | 20 | 13 | * | * | * | 21 | * | 10 | |
| Heart Failure | Elective | 23 | 120 | 63 | 34 | 23 | 115 | 14 | 14 |
| Emergency | 400 | 841 | 316 | 179 | 346 | 785 | 258 | 194 | |
| Other | 74 | 82 | 35 | 30 | 17 | 108 | 8 | 42 | |
| Stroke | Elective | 44 | 112 | 47 | 18 | 47 | 100 | 32 | 23 |
| Emergency | 626 | 1621 | 665 | 403 | 553 | 1531 | 404 | 306 | |
| Other | 252 | 486 | 191 | 150 | 145 | 519 | 106 | 103 |
Source: Secondary Uses Services, Commissioning Dataset, Inpatient Table, 2015
The admission type ‘Other’ includes transfers * indicates less than six admissions
Figure 9.26 shows the pattern of hospital admissions in the wider Devon area by age, sex and deprivation. The following patterns are seen:
- For the pattern by sex, only Asthma has higher prevalence in females. The conditions where male rates are particularly higher are CHD (181% higher).
- The pattern by age, generally highlights an increasing pattern with age, different patterns are Asthma and Epilepsy which both have younger peaks, and Diabetes which has a secondary peak for children aged 5 to 19.
- For all conditions admissions rates are higher in more deprived areas, which is particularly marked for COPD (299% higher) and Diabetes (222% higher). A stronger relationship with deprivation is seen for admissions compared to treated prevalence, highlighting the greater likelihood of ill health and complications in these groups.
Figure 9.26, Direct age standardised rate per 100,000 of hospital admissions (primary diagnosis only) for selected long-term conditions in Devon, Plymouth and Torbay, with summary breakdowns by age, sex and deprivation, 2011-12 to 2013-14
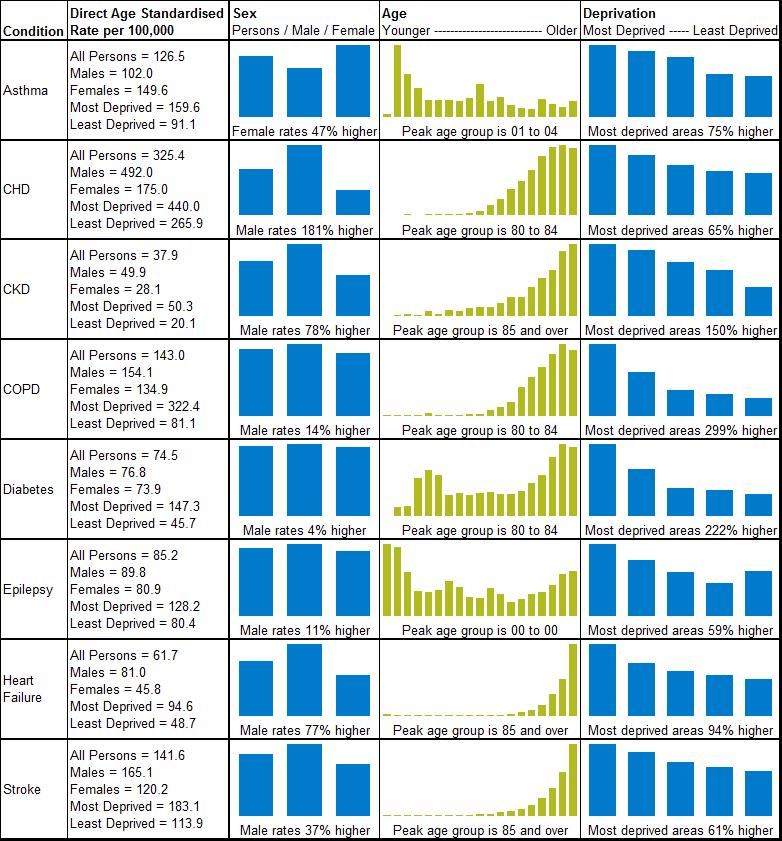
Source: Secondary Uses Services, Commissioning Dataset, Inpatient Table, 2015
| Box 4, Long-Term Conditions, Perceptions and Experiences
Healthwatch Devon undertook a survey of people living with long-term conditions in the county, which yielded 566 responses. The majority (63%) considered the care and support they received was good or excellent. “…a good combination of day-to-day care from GP practice, with well-defined routes to more specialist care as and when I need it.” Around two thirds were involved in decisions about their care, had enough information to manage their health, felt information provided was clear, had confidence in taking care of their own health or felt they had control over their care most of the time. “I am listened to when I have a problem with the existing regime of medication, but there is no systematic, regular review.” However, just under a fifth of respondents (18%) considered the care they received to be poor or very poor. Communication between mental and physical health services was highlighted as a particular area for concern, and concerns were also expressed about the sharing of information between health and social care services. “The support varies between average and poor. Both my carer and myself feel isolated at times in seeking information and support.” “More continuity would be good.” “Agencies do not seem to liaise with each other over my varying health problems, or keeping my family informed.” Two out of three respondents did not have a personal care plan, of which 95% had not talked it over with a professional. People highlighted communication, treating people as equal partners in their care, and holistic care were particularly important. “You are helped at first and then left to your own devices.” “Look at all aspects of my health and have a holistic plan where all health professionals involved work together.” Source Healthwatch Devon, ‘People Living with Long Term Conditions’ Report, December 2014 http://www.healthwatchdevon.co.uk/long-term-conditions/ |