Mental health and emotional well-being describes how we think, feel and relate to ourselves and others and how we interpret the world around us. Having good mental health affects our capacity to manage, communicate, and form and sustain relationships. It also affects our ability to cope with change and major life events.
Most people will come into contact with mental health issues during their lifetime, and one in four will have personal experience of a mental health problem. The invisibility of mental illness means many do not receive the support and treatment that could help them.
The Mental Health Foundation has highlighted some of the common mental health problems in childhood:
- Depression affects more children and young people today than in the last few decades, but it is still more common in adults. Teenagers are more likely to experience depression than young children.
- Self-harm is a very common problem among young people. Some people find it helps them manage intense emotional pain if they harm themselves, through cutting or burning, for example. They may not wish to take their own life.
- Children and young people with generalised anxiety disorder (GAD) become extremely worried. Very young children or children starting or moving school may have separation anxiety.
- Post-traumatic stress disorder can follow physical or sexual abuse, witnessing something extremely frightening of traumatising, being the victim of violence or severe bullying or surviving a disaster.
- Children who are consistently overactive (‘hyperactive’), behave impulsively and have difficulty paying attention may have Attention Deficit Hyperactivity Disorder (ADHD) Many more boys than girls are affected, but the cause of ADHD isn’t fully understood.
- Eating disorders usually start in the teenage years and are more common in girls than boys. The number of young people who develop an eating disorder is small, but eating disorders such as anorexia nervosa and bulimia nervosa can have serious consequences for their physical health and development.
Nationally there has been an increased prevalence of mental ill health in children and young people, with only a small proportion with mental health problems in contact with mental health services. Around one in 10 children in Devon have a mental health disorder.
The table below show the number of school-age children estimated to have a mental health condition by local authority district.
Table 8.9, Estimated number of school-age children (aged 5 to 16) with a mental health disorder, 2013
| Local Authority | Total |
| East Devon | 1,538 |
| Exeter | 1,398 |
| Mid Devon | 1,041 |
| North Devon | 1,185 |
| South Hams | 1,006 |
| Teignbridge | 1,521 |
| Torridge | 772 |
| West Devon | 672 |
| Devon Total | 9,133 |
Source: Association for Young People’s Health: Key Data on Adolescence 2013
Tier four specialist inpatient and day-patient care are for children who are suffering from severe and/or complex mental health conditions that cannot be adequately treated by community mental health services. According to the CAMHS Annual Report to the Devon Safeguarding Children’s Board, between 15 and 25 young people from Devon will be in inpatient care at any one time.
The range and nature of risk behaviour from young people at tier four is broad and can include self-harm, suicide, physical consequences of low weight, absconding, aggression, sexualised behaviour, fire-setting, and safeguarding concerns. All of these can represent a risk to the young person and may represent a risk to other patients. These risks and behaviours are harder to manage if the young person is placed on a paediatric ward instead of in a specialist Children and Adolescent Mental Health Services (CAMHS) bed.
There has been an increase within Devon of young people admitted to paediatric wards and to tier four units. Devon does not have specialist mental health beds in county (the nearest being in Plymouth, though the young people may be placed at a much greater distance if a more local bed is not available) meaning the majority of South West admissions have been to paediatric a ward on which staff may not have the specialist skills to support a mental health crisis. This means young people in crisis are being placed at great distances from their family and support networks and family members are unable to participate in supportive therapy.
Self-Harm
Self-harm amongst younger people is one of the most direct forms of impairment to health or development. It includes overdoses (self-poisoning) and self-mutilation, such as cutting, burning, and scalding. Self-harm can also be indicative of other underlying safeguarding
issues, such as those outlined in the protection from maltreatment sub-section. Reliable figures on the prevalence of self-harming are difficult to obtain, although work by the Social Care Institute for Excellence, suggest around 1% of children with a mental health problem self-harm (http://www.scie.org.uk/publications/briefings/briefing16/). In Devon, 139 males and 409 females aged 0 to 19 attending accident and emergency departments as a consequence of self-harm in 2013/14. Attendance rates peak in the 15 to 19 age group as illustrated in the chart below.
Figure 8.13, Accident and Emergency and Minor Injury Unit Attendance Rates for Self-Harm by Age Group, Devon, 2013-14
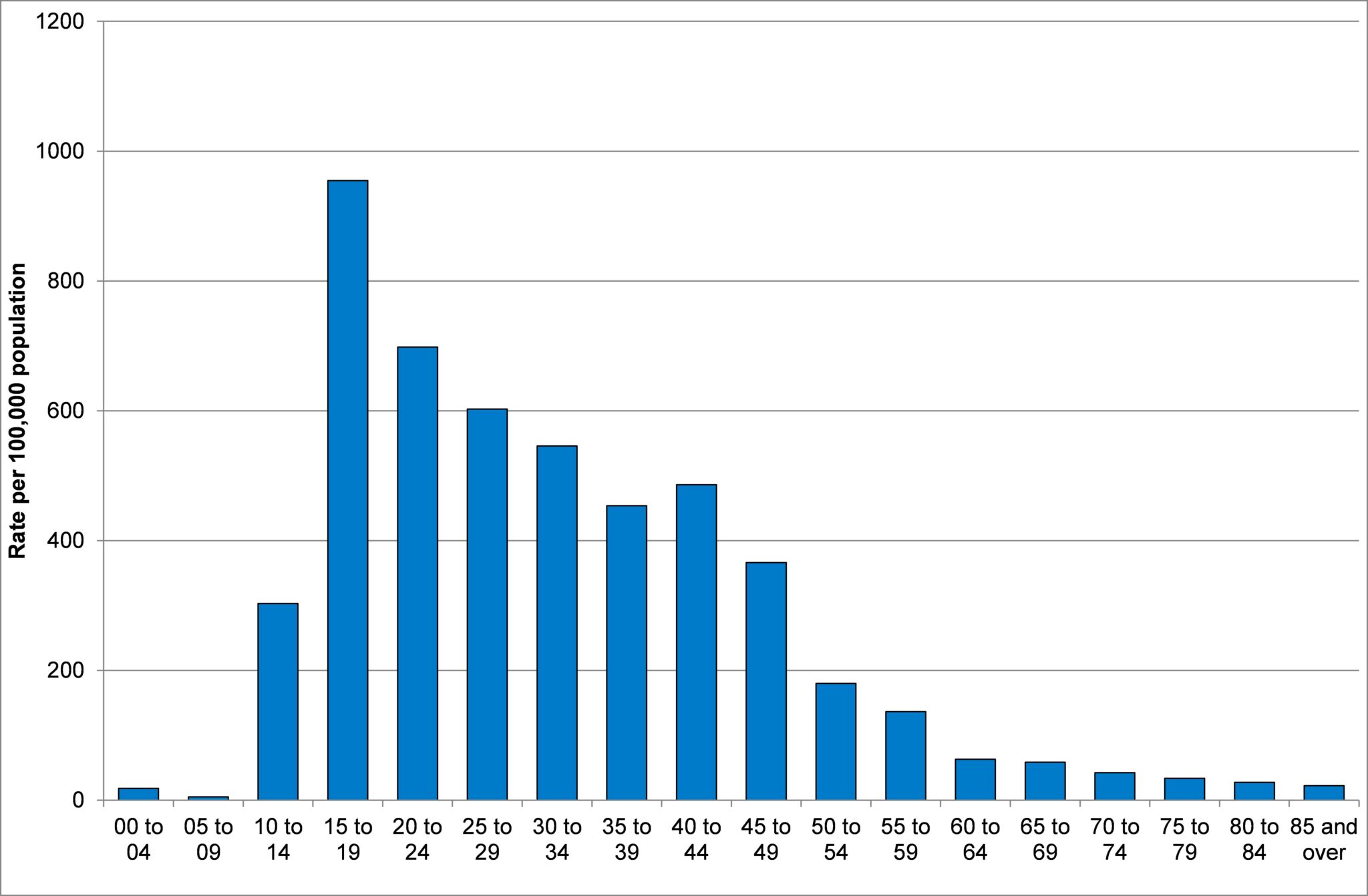
Source: Secondary Uses Service, Accident and Emergency Commissioning Dataset, 2014
The Child Health and Maternity Service (CHIMAT) monitor self-harm admissions in the 10 to 24 age group. There were 548 hospital admissions for self-harm in persons aged 10 to 24 in Devon in 2012-13. The rate per 100,000 in Devon was 419.5, which is below the South West rate (442.5), but above the local authority comparator group (388.8) and England (346.3) rates. Admission rates increased from 376.6 in 2007-08 to 419.5 in 2012-13. Within the 10 to 24 age group admission rates were highest in those aged 15 to 19 (625.4). Admission rates also are higher in more deprived areas, with a rate of 1034.0 in the most deprived areas compared with 308.6 in the least deprived areas in 2012-13. Within Devon rates were highest in North Devon, and lowest in the South Hams and Torridge. Rates of hospital admission for self-harm are three times higher in females than males and the gap has widened in recent years as illustrated in figure 8.14 below.
Figure 8.14, Hospital Admissions for Self-Harm by Year and Sex, Rate per 100,000 population, Persons aged 10 to 24, Devon
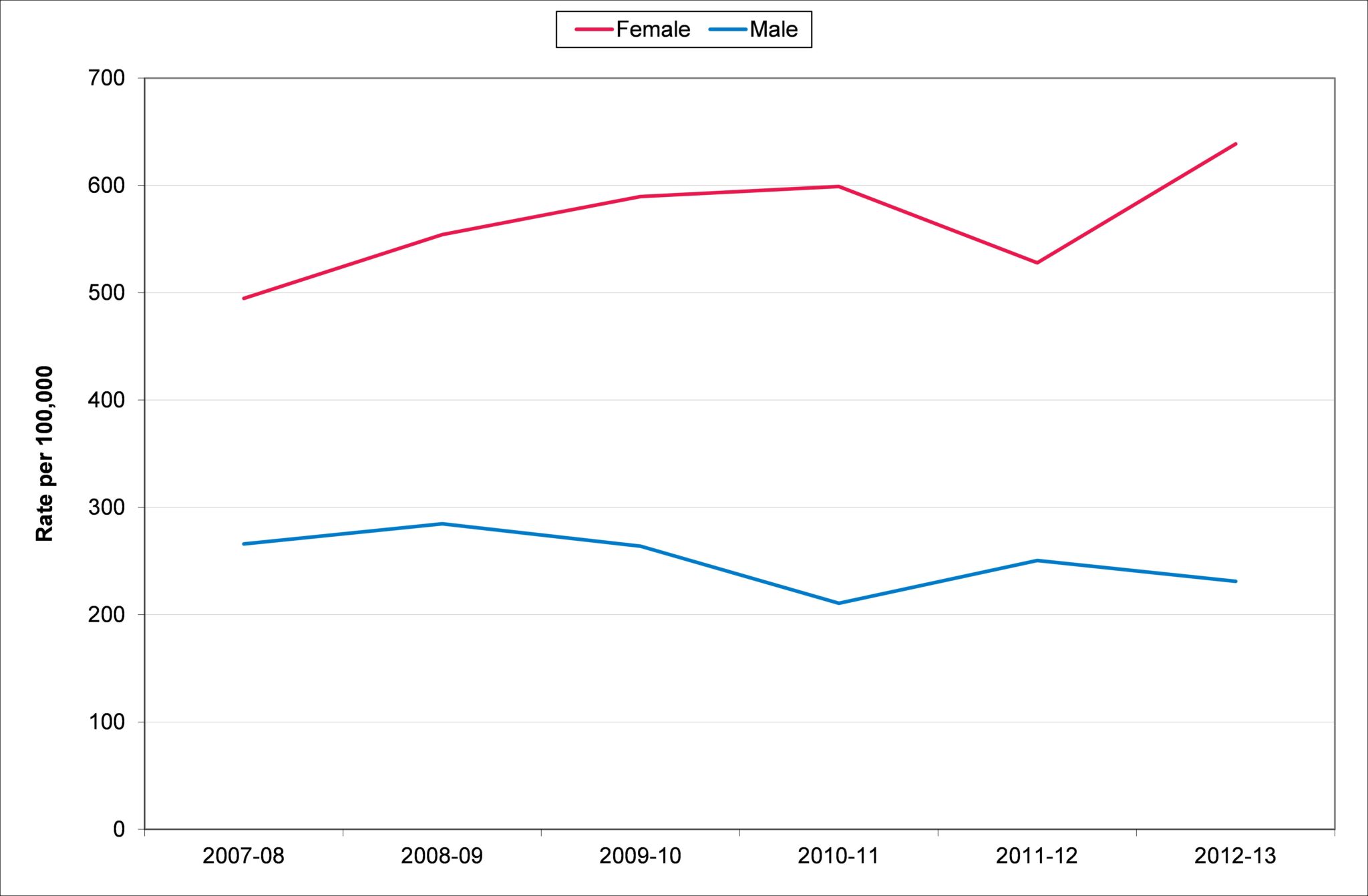
Source: Secondary Uses Service, Inpatient Commissioning Dataset, 2014
Eating Disorders
Eating disorders usually start in the teenage years and are more common in girls than boys. The number of young people who develop an eating disorder is small, but eating disorders such as Anorexia Nervosa and Bulimia Nervosa can have serious consequences for their physical health and development. Table 8.10 highlights around 122 persons aged between 11 and 15 have an eating disorder. Around 15 new cases of Anorexia Nervosa and 17 new cases of Bulimia Nervosa are expected in Devon each year.
Table 8.10, Estimated Incidence and Prevalence of Eating Disorders in Devon, 2013
| Condition | Rate | Numbers Affected in Devon |
| New cases of Anorexia Nervosa per year, aged 10 to 19 | 17.5 per 100,000 | 15 |
| New cases of Bulimia Nervosa per year, aged 10 to 19 | 20.5 per 100,000 | 17 |
| Persons with any eating disorders, aged 11 to 15 | 300 per 100,000 | 122 |
Source: Early Onset Eating Disorders, BPSU 2007 and LHO Mental Health of Adolescents 2000
Emotional Wellbeing of Looked After Children
The difficulties score is collected through a strengths and difficulties questionnaire, with higher scores (on a scale of 0 to 40) highlighting greater difficulties. The average difficulty score in Devon was 15.2 compared which is higher than the South West (14.8), local authority comparator group (14.3) and England (13.8) averages. The average score has decreased since 2011-12 level and the gap to the regional and national average scores has lowered. Difficulties score tends to increase with age with teenagers having higher difficulties scores. The older age profile of children in care in Devon may well influence the higher average scores observed.
Figure 8.15, Average of total difficulties score for all looked after children aged between four and 16 (inclusive) at the date of their latest assessment, who have been in care for at least 12 months on 31 March, Devon Local Authority Comparator Group, 2014
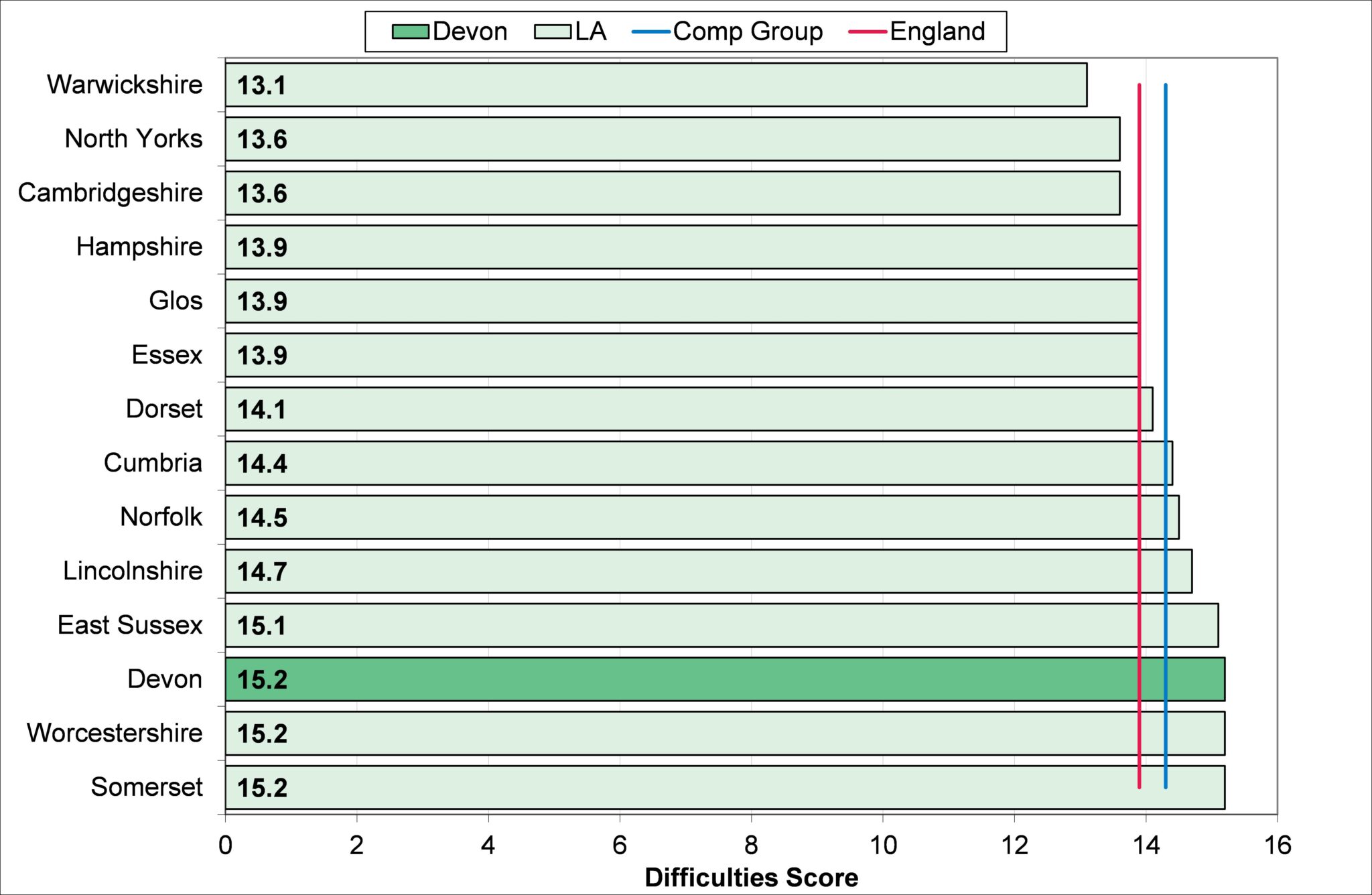
Source: Public Health Outcomes Tool, 2015